Introduction to adverse pregnancy outcomes
In 1931 Galloway first suggested that maternal periodontal infection may play a role in complications of pregnancy, including ”miscarriage, pyelitis, mastitis, phlebitis, anemia and toxemias of pregnancy” 1. Since then, evidence has accumulated linking the maternal periodontal disease with adverse pregnancy outcomes. In the last decade, the adverse effects of periodontitis on pregnancy outcomes have gathered a lot of attention. Presently, adverse pregnancy outcomes that have been linked to periodontal disease include preterm birth, low birth weight, miscarriage or early pregnancy loss, and pre-eclampsia. Pre-eclampsia and preterm births are major causes of maternal and perinatal morbidity and mortality 2, 3. In the following discussion, we shall study various aspects of periodontitis and adverse pregnancy outcomes.
Physiology of normal pregnancy
To understand how periodontal pathogens may affect the pregnancy outcomes, we should know the normal physiology of pregnancy. Pregnancy is characterized by progesterone-mediated hyperemia and edema of mucosal surfaces. After conception, the placenta that originates from the fetus invades and grows supported completely by the maternal uterine tissue. The umbilical cord connects the fetus with placenta and is responsible for the exchange of nutrients and waste between the mother and the fetus. The fetus grows in the amniotic fluid in the amniotic sac. The walls of this cavity consist of the amnion and the chorion. As the uterus enlarges by about 20 weeks’ gestation, the supine position may result in significant compression of the inferior vena cava, or supine hypotension syndrome. This uterine compression may ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book………….
During the course of pregnancy, the diaphragm is displaced cephalad about 4 cm, and the lower chest wall widens about 5 to 7 cm. These changes peak at 37 weeks’ gestation, which is important if the patient requires a chest drain. When the diaphragm is pushed upward, the heart is rotated slightly to the left, which results in electrocardiographic changes of Q waves inferiorly along with T-wave inversion. Blood pressure, especially the diastolic component, tends to be lower in pregnancy. Physical examination often reveals a systolic ejection murmur and a third heart sound.
As the pregnancy progresses, the fetus grows in size and its nutrients needs increase. Along with this, the decreasing space becomes a critical parameter that plays an important role in parturition. As the pregnancy progresses, amniotic fluid levels of prostaglandin E2 (PGE2) and inflammatory cytokines, such as TNF-α and IL-1β rise steadily until a critical threshold level is reached to induce rupture of the amniotic sac membranes, uterine contraction, cervical dilation and delivery 4. Hence, it is important to understand here that the parturition process is controlled by various pro-inflammatory cytokines and abnormal changes in their levels in the amniotic fluid may affect this process.
Changes in periodontal microflora during pregnancy
There are many physiological hormonal changes that occur during pregnancy. Estrogen and progesterone are the main pregnancy sex hormones. Their level rises until the eighth month of pregnancy and after that, it becomes stable until birth. The estrogen level rises slowly until the end of pregnancy 5. Gingival inflammation associated with pregnancy that has been initiated by dental plaque is exacerbated by these endogenous steroid hormones. There are significant changes in the subgingival microbiota in pregnant patients. Kornman and Loesche (1980) 6 were the first to report statistically significant increases in the levels of Bacteroides intermedius during the second trimester, with a reduction during the third trimester and after delivery. This increase in the levels of Bacteroides intermedius was associated with increased serum levels of progesterone or estrogens which substituted for the naphthoquinone requirement of the pathogens and thus acted as a growth factor for the bacteria . De-Albornoz et al. (2010) 7 observed ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book………….

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Adverse pregnancy outcomes
Preterm and low birthweight:
Birth weight is an important parameter for the chances of a newborn infant to survive, grow and develop healthily. The normal birth weight varies from population to population and race to race. It is important to note here that birthweight is an unrefined measure of fetal growth; babies may have the same weight but differ in length and proportion of fat.
First of all, let us try to understand, what is preterm and low birth weight? The international definition of low birth weight adopted by the Twenty-ninth World Health Assembly in 1976 is a birthweight of ”less than 2500 g” (up to and including 2499 g) 9. Below this value, birthweight-specific infant mortality begins to rise rapidly. There are two reasons for low birthweight: premature birth and retarded intrauterine growth of the fetus. The preterm or premature birth is usually defined as ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book………….
Preeclampsia:
Preeclampsia is a pregnancy-specific disorder that affects 3-5% of females. It results from a “sick” placenta. This condition affects primarily the pregnant woman instead of the fetus. Defective invasion of the spiral arteries by cytotrophoblast cells is observed during pre-eclampsia. Further, in this condition, the smooth muscles of spiral arterioles is not replaced by hyaline material. The clinical picture of this condition is wide. The condition is clinically manifested as headaches, tinnitus, phosphene signals, visual disorders, brisk tendon reflexes, and vigilance disorders (related to cerebral edema); oliguria to acute renal failure; uterine contraction, vaginal bleeding to placental abruption, epigastric pain and cardiac failure.
Miscarriage:
A miscarriage is the loss of a fetus before the 20th week of pregnancy. It is one of the most common complications associated with early pregnancy. Most miscarriages occur during the first few months of pregnancy. An estimated 85 percent of miscarriages happen before week 12. It has been observed that periodontal diseases appear to be associated with miscarriage between 12 and 24 weeks of gestation, even after controlling for other risk factors of poor pregnancy outcome 11. However, it is not yet known whether treating periodontal disease in pregnancy can reduce the risk of miscarriage.
Intrauterine growth restriction (IUGR):
IUGR is defined as a fetus that fails to achieve his growth potential. It affects 3-10% of pregnancies and 20% of stillborn infants have IUGR. Perinatal mortality rates are 4-8 times higher for growth-retarded infants, and morbidity is present in 50% of surviving infants. The risk factors for IUGR include chromosomal abnormalities 12, 13, multifactorial congenital malformations 14, multiple gestations 15 and fetal infections. There are only a few studies on the association of periodontitis with IUGR. Siqueira et al. (2007) 16 did a study on ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book………….
Mechanisms relating periodontitis to adverse pregnancy outcomes
Three mechanisms have been postulated whereby periodontal disease may cause pregnancy complications. All these mechanisms are related to the ingress of various metabolically active products of the bacterial and host origin (resulting from host-microbial interactions) into the maternal systemic circulation. These three proposed mechanisms are,
Lipopolysaccharides (LPS) from the Gram-negative bacteria entering the systemic circulation:
LPS derived from various Gram-negative periodontal pathogens may enter the systemic circulation and target the uterus and placental membranes. LPS are strong inducers of IL-1β and prostaglandin E2 (PGE2) production by chorio-amniotic and trophoblastic cells. This process is associated with preterm parturition. It has been demonstrated in the animal studies that bacterial LPS have adverse effects on pregnancy outcomes. In an experiment on pregnant golden hamster, the intravenous injection of P. gingivalis LPS resulted in fetal growth restriction and fetal resorption 17, 18.
In another experiment on sheep model, it was observed that injection of LPS from Escherichia coli into the amniotic cavity causes inflammation of the fetal membranes, moderate systemic inflammatory responses in the fetus, and profound maturation of the lungs 19. Newnham et al. (2005) 20 have demonstrated ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book………….
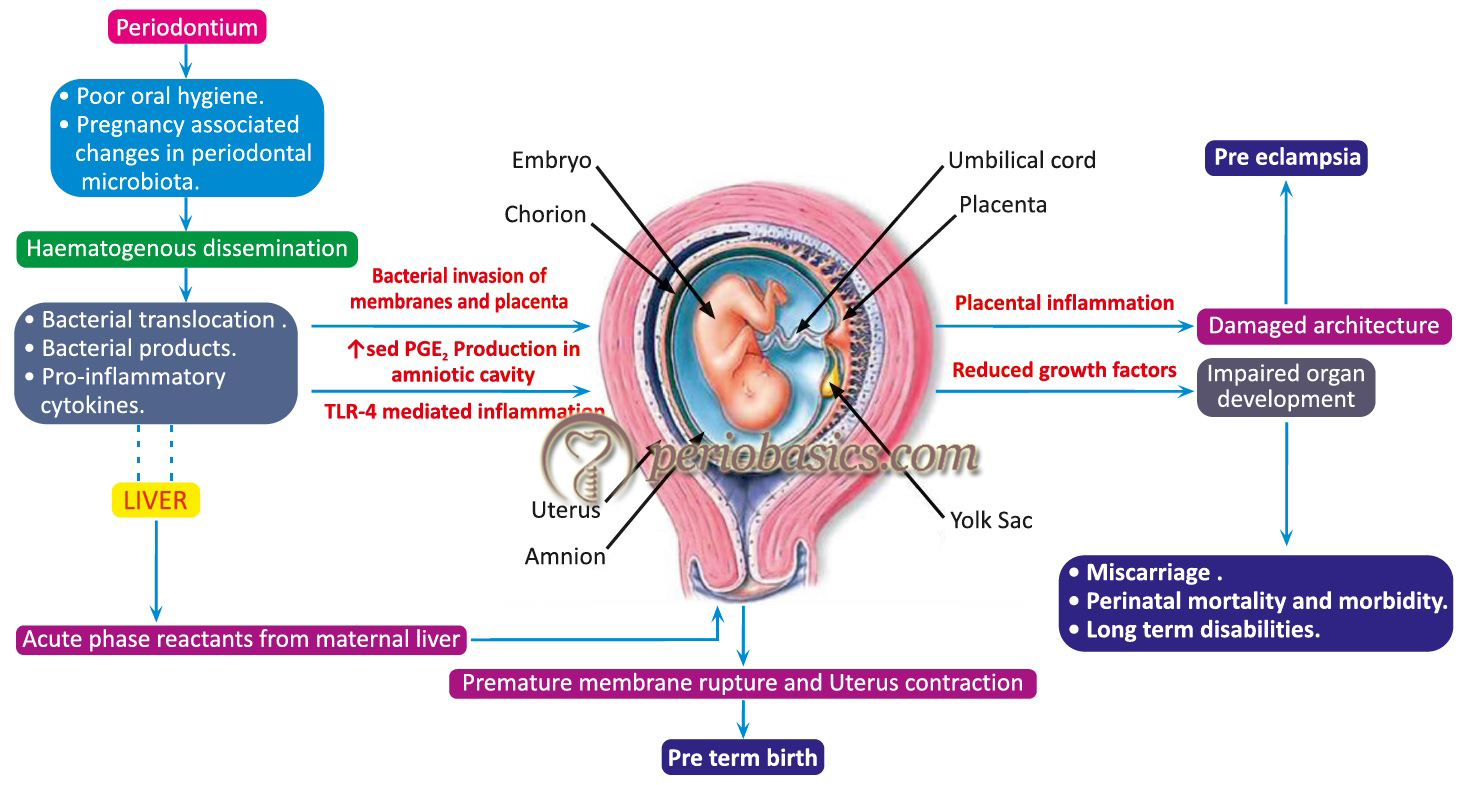
Role of proinflammatory cytokines and prostaglandins:
It is a well-established fact that due to the presence of periodontal pathogens in the plaque biofilm, various pro-inflammatory mediators are produced due to host-microbial interactions. The host immune cells such as neutrophils, macrophages, monocytes, mast cells, and epithelial cells secrete various chemical mediators that potentiate the inflammatory process in that arena. It should be remembered here, that both pro- and anti-inflammatory chemical mediators are active in the area of infection but due to the constant presence of putative pathogens, the pro-inflammatory mediators have an upper hand. Cytokines such as IL-1β, IL-6, and TNF-α together with PGE2 are produced locally within the periodontal pocket. These can be detected in the gingival crevicular fluid. However, due to the high vascularity of the periodontium, these mediators may act as a potential source of systemic inflammation and oxidative stress.
Damare et al. (1997) 21 did a study on pregnant women with periodontal disease undergoing amniocentesis in the second trimester. The authors found that levels of PGE2 and IL-1β in gingival crevicular fluid correlated with levels of the same two agents in amniotic fluid in mid-trimester. Unfortunately, pregnancy outcome data were not available for this group of women. The levels of IL-6 and PGE2 have also been found to be elevated in amniotic fluid in the mid-trimester in women with periodontal disease. These increased levels were found to be associated with increased rates of preterm birth 22. The increased levels of ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book………….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Bacterial translocation from oral cavity:
Bacterial translocation from the oral cavity may be associated with adverse pregnancy outcomes. The most common bacterium cultured from amniotic fluid in human preterm labor is F. nucleatum which is strongly associated with periodontal disease 23. In one study, it was observed that after intravenous injection of F. nucleatum in pregnant mice, the bacterium could be isolated from the uterus, membranes, and amniotic fluid, despite not being detected in maternal viscera 24. In a large case-control study on women with severe periodontal diseases and preterm birth, very few placental cultures were found positive for periodontal organisms, despite meticulous culture techniques of these fastidious organisms 25. These findings suggest that bacterial translocation may not be a common mechanism, relating periodontitis and adverse pregnancy outcomes.
Review of literature
The dissemination of bacterial products and bacteria themselves in the systemic circulation and their subsequent colonization in the amniotic/feto-placental tissues have been studied well. P. gingivalis and Aggregatibacter actinomycetemcomitans have also been found in the placenta of women with preterm birth or pre-eclampsia 26-28. One more un-cultivated oral bacteria that was found in amniotic fluid is Bergeyella 29. Han et al. (2010) 30 in one case report found F. nucleatum as the cause of a term stillbirth and was isolated from the lung and stomach of the infant. Interestingly, the same clonal type of F. nucleatum was present in the subgingival plaque of the mother, but not in her vaginal or rectal microflora. F. nucleatum is also one of the most common isolates from the amniotic fluid of patients with preterm low birthweight. This organism has also been detected in chorionic tissues of high-risk pregnant women 31, 32. P. gingivalis, F. nucleatum, and Capnocytophaga have been found in neonatal gastric aspirates obtained from complicated pregnancies which indicated the translocation of these periodontal pathogens in the fetal organs 33, 34.
As already discussed, various chemical mediators have been studied for their association with adverse pregnancy outcomes. Out of all the studied chemical mediators, elevated levels of IL-1β, IL-6, TNF-α, PGE2, fibronectin, and α-fetoprotein in the amniotic fluid have been associated with preterm birth. Other biomarkers such as MMPs, estriol, elastase, protease, phospholipase, prolactin myeloperoxidase and tissue inhibitor of MMP (TIMP)-1 have been evaluated but no conclusive results could be drawn 35, 36. Many studies have demonstrated the elevated levels of maternal serum levels of pro-inflammatory cytokines, such as IL-1, IL-6, IL-8 and TNF-α and their association with preterm low birthweight 37-41. Along with these ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book………….
Conclusion
The adverse effect of periodontal diseases on pregnancy outcomes has been well documented. In the above discussion, we addressed various aspects of this relationship. The emerging intervention studies have reported that performing scaling and root planing in pregnant women with periodontitis may reduce pre-term births. These findings demand more research in this field of periodontal medicine. Along with this, the healthcare providers for pregnant women should understand the importance of maintenance of oral hygiene for the betterment of both the mother and the child.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.